Inclusion is a wonderful thing – and we should all want a world where inclusion is valued, and everybody can be part of public life and free to live without stigma. However, inclusion should not involve erasing or misrepresenting the needs of marginalised groups of people, tokenising their existence, without trying to understand their needs – especially when their needs are diverse and complex and not easily boiled down to a single letter.
The I does not stand for Invisible!
So, I would ask all organisations adding the I, do you really understand what this stands for and are you really trying to improve the lives of people living with variations of sex development? Or are you just adding the I because you think this is the best way to look “inclusive”, whilst ignoring their actual needs?
The I also does not stand for Ignoring needs!
I have written in detail about the term intersex https://differently-normal.com/2021/10/25/the-invention-of-intersex/?preview_id=292&preview_nonce=9f62da2a5a&preview=true and probably the first thing to note, is that the majority of people who are living with differences of sex development, do not identify as intersex, may not know the term is used to describe their medical history and may even find the term difficult or even stigmatising. It is also increasingly common for people without a DSD, to identify as intersex, with even Polycystic Ovarian Syndrome being claimed as the most common intersex variation, even though most women with PCOS would never describe themselves as intersex and this is not officially recognised by any medical organisation.
So, when adding the I, who are you representing?
1) People without a DSD who choose to identify as intersex – or
2) those with a DSD, who may not use or even like the term?
By adding the I, are you erasing the needs of the most vulnerable, including newly diagnosed children and instead prioritising the needs of people who see “intersex” as an identity, for ever more spurious reasons?
So, let’s think about needs?
Surely any genuinely inclusive organisation would want to consider the needs of the most vulnerable as a priority – and when this comes to the I, surely this would prioritise the 0.2% living with complex differences of sex development. Some of these conditions are listed below:
Klinefelter’s Syndrome
Turner Syndrome
Mixed Gonadal Dysgenesis (Mosacism)
Complete Gonadal Dysgenesis
Partial Gonadal Dysgenesis
Frasier Syndrome
5-alpha reductase deficiency
17-beta deficiency
Complete Androgen Insensitivity Syndrome
Partial Androgen Insensitivity Syndrome
Persistent Mullerian Duct Syndrome
Ovostesticular DSD
Congenital Adrenal Hyperplasia
Mayer-Rokitansky-Kuster Hauser (MRKH) syndrome
If your organisation does not know the names and does not understand the needs of people living with these complex conditions, are you in any way able to advocate for them?
Did you know that Turner syndrome can be associated with significant heart and kidney problems – or that Klinefelter’s can increase the risk of developing Type 2 diabetes or osteoporosis?
Does your organisation understand that girls with MRKH or Complete Androgen Insensitivity Syndrome, may find out as young teens that they were born without a uterus and with a short vagina and that this can impact on both fertility and sexual function? Can you provide information about options for vaginal hypoplasia, which can include dilators and surgery? Can you provide the psychological support needed to come to terms with this information? Are you aware that she may find her bodily difference being described as “intersex”, incredibly difficult – especially if this is done as part of “inclusivity” training and without understanding anything about her needs?
It may be especially difficult for a young teen, to be faced with their bodily difference being described as neither male or female, as is frequently suggested by lessons using the GenderBread person. Is this genuinely being “inclusive”, or is this using a vulnerable group of people without considering their needs – and without engaging with expert advice as detailed here. https://dsdfamilies.org/application/files/9116/3519/2768/July_2021_schools.pdf
Does your organisation know that every year in the UK, around 150 babies are born with complex genital difference? This can be associated with a number of life threatening and life limiting syndromes and further investigations may be needed to determine the cause and in rare cases, whether best to raise baby as a boy or a girl? Do you offer support to new parents facing these issues, so that they are able to advocate for their children? Are you aware that labelling these babies as neither male or female or a third sex, can increase the risk of unnecessary surgeries? Do you provide funding so that parents are equipped with the skills to raise confident children living with different bodies?
Does your organisation know that one of the most common causes of atypical genitalia, Congenital Adrenal Hyperplasia (CAH), is a medical emergency and associated with the possibility of a life-threatening adrenal crisis? Babies can develop arrhythmias, vomiting and dehydration shortly after birth and will need lifelong medication. What support and information do you offer to these families – and does your organisation understand that the overwhelming majority of people with CAH, reject the term intersex? Does your organisation understand that someone with CAH may be sitting in your “inclusivity” training and may be distressed by how you are describing their bodily difference?
When adding the I, without really understanding the I, are you misrepresenting the needs and bodies of people born with variations of sex developments and adding to public confusion? Are you contributing to these conditions being weaponised and turned into memes that are used to discuss issues around sex and gender, without any genuine interest in needs? Do you consider that there are likely people working in your organisation, who are living with these complex conditions and may find it traumatic to have their medical conditions misrepresented?
Most importantly, when adding the I, are you removing funding opportunities from the most at need – and are you preventing funding being available to meet the needs of those who are living with complex variations of sex development?
If by adding the I, you are genuinely wanting to improve the lives of people born with variations of sex development, we need more than just a hashtag – we need funding and services that prioritise our healthcare and psychological support. If you genuinely want to be inclusive, do not misrepresent or ignore the voices of the people you are claiming to support – and do not add the I without first listening and understanding our needs.
If you are claiming to stand against interphobia and really want to end discrimination, please start by ensuring you don’t make the I invisible by ignoring our needs.
And finally, if you are serious about inclusion and your organisation really believes that we are more than just a hashtag, consider donating to our needs https://dsdfamilies.org/donate
The below essay is very quickly written and still very much a work in progress, but I felt it was important to share some of this information as part of Intersex Awareness Day.
As someone born with Complete Androgen Insensitivity Syndrome, I had until recently felt fairly neutral about the term Intersex as I could see its value as a political label and as a way of understanding the bodies of those of us living with complex variations of sex development – and I have found it amazing to see young activists embracing and celebrating their bodily differences under an intersex flag.
However, the recent appropriation, misrepresentation and even fetishizing of ‘intersex’ has led to me increasingly believing that the term is doing more harm than good.
I am also increasingly contacted by young people, adults and new parents that have never met anyone else with the same variation of sex development, possibly as they do not feel represented by current activism that focuses only on those who identify as intersex. Peer support can be hugely valuable – and I would like this to be available for all, regardless of how they identify.
I do not mean this essay to be a criticism of people using the term intersex to describe themselves, however, I am critical of using intersex to describe babies and children, who do not have a choice.
Does the I need to be more Inclusive?
On Intersex Awareness Day, I want to start with what has sadly become a controversial statement.
I want to support ALL people born with variations or differences of sex development (DSD) and not only those who choose to identify as intersex. I want to ensure that all children born with differences in their sex or reproductive development, get the family, psychological and peer support they need, to make informed choices about their healthcare. Most importantly, I want them to have access to accurate and precise information about their bodies and to have the opportunity to meet other young people who share their experience.
For this to be possible, there needs to be activism, advocacy and academic research that is truly inclusive and centres the children and families most in need of support – and listens to a diverse range of voices and not only to adults who identify as intersex.
What even is Intersex?
Even the definition of intersex is contentious, poorly understood and defined – and although the lack of a clear definition is often explained as being ‘inclusive’, this is frequently leading to the children most in need of support, being lost in a sea of debates about gender identities or whether or not sex is a binary, bimodal or a spectrum. Every single part of the body can vary in shape, size, and function – and this can vary from slight cosmetic difference to life threatening complications. This is no different when considering variations in the development of the reproductive system – and yet differences associated with this part of the body are increasingly politicised and presented as an identity, that you can choose even without any anatomical difference.
Prior to the 2006 Chicago Consensus Meeting/Statement, the term intersex usually only applied to the 0.02% of the population, living with the most complex variations of sex development, as detailed in the figure below.
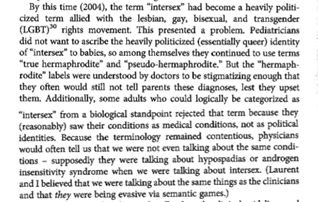
The term Disorders or Differences of Sex Development (DSD) was proposed to replace the previous umbrella terms that included, True Hermaphrodite, Male Pseudo-hermaphrodite, Female Pseudo-hermaphrodite and Intersex – as many parents and patients had criticised the terms as being stigmatising and out of date, as well as the automatic associations with being “between the two sexes”. The term DSD also allowed the inclusion of conditions such as MRKH, that share many common features. Using the word disorder was criticised, including by the representatives of the AIS Support Group in the UK http://web.archive.org/web/20170117130415/http://www.aissg.org/15_ANNOUNCE.HTM#16%20Aug%202006 and they suggested that difference, diverse or variation of sex development may have been better options and difference or diverse has increasingly replaced disorder in research and patient information.
Although the term DSD is frequently used within medical research, most healthcare providers use condition specific language when talking to patients and their families – and this is usually preferred by people living with variations of sex development, possibly as this is the most useful way for them to describe and understand their bodily differences.
However, although the term intersex is not used by most people born with a variation of sex development, many activist and support groups have intersex as part of their name – and can be critical or even hostile to anyone using DSD terminology. Although I can understand that some adults strongly identify as intersex, not creating a space for people who view things differently, for example seeing themselves as someone with a medical condition, can result in many people feeling excluded from the groups that are supposed to support and centre their needs.
Possibly as a way to feel that they are being inclusive, intersex groups, academics and policy makers have changed the definition of intersex to include an ever widening group of people – and increasingly imply that intersex is an identity that is open to everyone, even based on an internal feeling.
The most common statistic used in the media, is the 1.7% from Anne Fausto-Sterling, https://onlinelibrary.wiley.com/doi/abs/10.1002/%28SICI%291520-6300%28200003/04%2912%3A2%3C151%3A%3AAID-AJHB1%3E3.0.CO%3B2-F which frequently leads to the statement that being intersex is as common as having red hair However, this does not clarify that the majority of the 1.7% have late onset CAH, which does not present with atypical sex development, but presents most commonly in adulthood in a similar way to Polycystic Ovary Syndrome (PCOS).
However Polycystic Ovaries has also been brought under the intersex umbrella and was the most common intersex condition in the Australian Research “Intersex Stories and Statistics”, which is frequently quoted in academic journals about intersex. https://ihra.org.au/30313/intersex-stories-statistics-australia/
The ILGA-Europe have gone one step further and define intersex as:
“Intersex individuals are born with physical sex characteristics that don’t fit medical or social norms for female or male bodies. The variations in sex characteristics may manifest themselves in primary characteristics such as the inner and outer genitalia, the chromosomal and hormonal structure) and /or secondary characteristics such as muscle mass, hair distribution and stature”https://www.ilga-europe.org/sites/default/files/Attachments/intersex_final_position.pdf
If intersex is referring to a variation in secondary sex characteristics, does this not make almost everyone in the world intersex at some level as detailed in the figure below? This may all sound lovely and inclusive, but it is likely to prevent the children and families most in need, from getting support and funding.
As well as intersex having no clear definition, the term is also frequently misunderstood to refer to gender identities. This was highlighted in the recent paper by Peter Hegarty https://psycnet.apa.org/record/2020-57692-001 that found the term intersex was frequently understood as referring to social or gender identities. Emi Koyama also noted that it was more common for people without a DSD to identify as intersex, than those with a DSD, who mainly see themselves as men and women with a medical condition. http://www.ipdx.org/articles/letter-outsidein.html
Self-identifying as intersex, without a DSD, is not uncommon https://www.tandfonline.com/doi/abs/10.1080/19317611.2011.629287?journalCode=wijs20 and this has a big impact on representation and research. The European Union for Fundamental Rights (FRA) recently ran a large survey asking people to self-identify as intersex. https://fra.europa.eu/en/publication/2020/eu-lgbti-survey-results The results from this survey, illustrated that only one third had a DSD diagnosis, one third had seen a doctor but given no diagnosis and one third had decided for themselves. Of this group, almost half of them had a diverse gender identity, including cross dresser, polygender and genderfluid.
This survey was not shared with any patient groups or healthcare professionals working within this field – and in the UK it was only shared with the groups below:
Birmingham LGBT
UKPON
Intersex UK
LGBT Consortium
Kaleidoscope Trust
PinkNews
Galop
G3 magazine
Mosaic
Rainbow Project
LGBT History Month
Scottish Trans Alliance
The Proud Trust
Fyne Times
LGBT Youth Scotland
The F Word
LGBTI Solidarity for Peoples of Turkey
Diva Magazine
Stonewall
EDF – Equality and Diversity Forum
Stonewall Scotland
Gay Star News
One Body One faith
Lancashire LGBT
UK Black Pride
TMSA UK
Imaan
LGBT Foundation
UK Lesbian and Gay Immigration Group
LGBT Youth Scotland
National LGBT Police Network
myGwork LGBT+ Business Community
Scottish LGBTI Police Association
Lesbians and Gays Support the Migrants
Mermaids
Equality Network
Gendered Intelligence
Bicon – conference about bisexuality
Switchboard
Student Pride
GIRES
Mind Out
Press For Change
And was not shared with dsdfamilies, Living with CAH, Turner Syndrome Support Group, Klinefelter’s Syndrome Association UK, MRKH UK Support – or any other UK patient support or advocacy groups or their European equivalents – or any healthcare teams. Although it is also vital to research the needs of gender diverse populations, this should not be at the expense of people with DSD.
Representatives from dsdfamilies met with the Cabinet Intersex Expert for the EU Commissioner for Equality, to discuss the exclusion of patient and family groups who used DSD terminology, from the research. We expressed our concern about the research not being representative of the needs of the people they claim to support and yet still being used to direct policy. For example, focusing on legal gender recognition above the need for good medical & psychological care – our concerns were dismissed as transphobia.
The above Intersex Expert had also produced this paper in 2015 https://book.coe.int/en/commissioner-for-human-rights/6683-pdf-human-rights-and-intersex-people.html that highlighted legal gender recognition as a priority issue for intersex people. There was little recognition of medical needs and the only reference to psychological care, seemed to conflate this with conversion therapy. This paper was criticised by people living with variations of sex development as well as experts working in this area https://www.europeanurology.com/article/S0302-2838(16)30179-8/fulltext but little seems to have changed – and similar self-selecting surveys are currently being used in many other areas.
This includes the LGBT report produced by the UK Government in 2017, that also relied on an online survey that asked people from LGBT groups to self-identify as intersex. This resulted in a response of 2000 people identifying as intersex (2% of respondents) – and the analysis acknowledged that this was likely not to be representative and that people were using the term “intersex” to mean something non-medical, possibly conflating with non-binary identities. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/721704/LGBT-survey-research-report.pdf
In contrast, when a dedicated Call for Evidence, open to all people with intersex/DSD and designed to ensure that responses were included from people with a diagnosed DSD, along with their families and professionals working with them, there were only around 300 responses – and the analysis of this information has still not been published.
The LGBT Survey led to a request by the Women and Equalities committee, ministers and some individuals and organisations, to find a way for people to use the Census to state that they were intersex. Following discussions with stakeholder and likely due to the Call for Evidence on ‘Intersex/DSD/VCS’ by the same Government Equality Office from 2019 only receiving 300-350 responses, the Sexual Orientation and Gender Identity department of ONS, supported by the National Statistician’s Data Ethics Advisory Committee, recommended against referencing ‘intersex’ in the Guidance of the Census.
Following our discussions with ONS we believe that this decision was made as there is no definition that allows a clear understanding of what/who is being measured, there is ‘no strong data user need’ and mixed views about ‘respondents need’, and a very clear understanding that data gathered will not be reliable and will not have any usability/value in terms of informing policy. At dsdfamilies, we are keen for ONS to go further and to commit to find other routes of gathering data around variations of sex development through the health department of ONS. This remains under discussion.
Currently, the Intersex Mapping Study in Ireland https://www.dcu.ie/intersex is also using a study design based on an online survey that asks people to self-identify as intersex. This is also likely to produce inaccurate and unreliable results – as the most important first step when designing any research project, is to accurately define the population you want to study. This is rarely done by academics working on intersex issues, which raises the concern that the work they produce, is misleading and does not represent the people most in need of support.
Choice of terminology
Academics from the social sciences, overwhelmingly use the term intersex, even though it has the potential to exclude many people born with variations of sex development, who only use DSD or condition specific language. The choice of language is often justified by the preference of activists – although sometimes misleading statistics are also used.
“In the nascent field of interdisciplinary intersex studies, terminology, and consequently definitions, have raised a number of difficulties. Whilst most activists and scholars prefer the term ‘intersex’, others, particularly medical professionals and those working in close partnership with them, have preferred the term ‘disorders of sex development’ (DSD – coined in 2006) or ‘differences of sex development (dsd)’.1 In 2015, Malta gave legal protection on the basis of ‘sex characteristics’, building traction for the use of the terminology ‘variations of sex characteristics’ (VSC) in legal and human rights discussion. However, it is worth reflecting on the fact that in her work in the UK and Sweden, Lundberg found that only a minority of young people with variations of sex characteristics had heard of the term ‘intersex’ (Lundberg, Hegarty and Roen 2018). Due to the pathologising connotations of the term DSD both for intersex people (Davis 2015) and for lay audiences (Hegarty et al. 2020), and the potential for VSC to be understood as both innate and acquired, this editorial will use the more common term intersex”
However, from looking at the references they provided to make this decision.
Lundberg – although only a minority of young people with variations of sex development had heard of the term ‘intersex’ – the above authors left out that only 10% of young people either liked the term or thought that they could use it. https://www.tandfonline.com/doi/full/10.1080/19419899.2018.1453862
Currently, the main issue discussed by intersex activists and academics, is the banning of early genital surgery. However, this has not been accompanied by a call for expert psychosocial services to offer family and peer support. Surgical interventions are also frequently discussed in the most crass and inaccurate ways, which has led to an increasingly simplistic and potentially stigmatising understanding of the complex issues involved, as highlighted by the recent comments by Eric Weinstein, that stated:
“intersex babies unfairly subjected to white coated physicians playing god with random irreversible sex changing surgeries without a scientific basis”.
A similar narrative is frequently presented in intersex academia – giving the lay person the impression that up to 1.7% of the population have their gender forcibly assigned by surgery and that doctors randomly assign a sex and that this is frequently wrong. This narrative possibly goes back to GIRES and their attempts to speak for the AIS support group in the UK http://web.archive.org/web/20170117130415/http://www.aissg.org/15_ANNOUNCE.HTM#14%20May%202000 – and their wish for the AIS support group to be involved with a documentary that was possibly going to use genital surgeries to address wider issues of ‘gender identity’. At this time, the AIS support group advised that they were against unnecessary surgeries on ethical, social and philosophical grounds, but that they didn’t have the experience as most of their members did not have genital surgery and that their priority issues were concerned with issues of truth disclosure, lack of emotional support, childhood gonadectomy without informed consent, osteoporosis, poor treatments for vaginal hypoplasia. However, these issues are now rarely discussed by academics or activists, who instead only talk about genital surgery – and often as a way to centre gender identities and gender recognition, even using inaccurate statistics to promote this narrative.
“In the case of intersex people, estimates of assigning the wrong sex to them vary between 8.5% and 40%. These children end up rejecting the sex they were assigned at birth demonstrating the major infringements of their psychological integrity”.
Firstly, the children in this study were not rejecting the sex they were assigned a birth and the study was only looking at whether they experienced any degree of gender dysphoria. Dysphoria may be understandable in the context of young people with atypical sex and reproductive development, especially if their body develops in unexpected ways during puberty – and should not be used to suggest a rejection of the sex they were assigned at birth.
Secondly, the study was a review of the literature and looked at 18 studies. 8 studies found no gender dysphoria present – and of the remaining studies, the range of dysphoria was between 8 and 20%, as the authors dismissed the one study that indicated a rate of 38%, as this included mainly patients with severe conditions such as cloacal exstrophy and penile agenesis, where significant confusion or distress about their body could be expected, regardless of sex of rearing.
For both CAH and hypospadias, there are good evidence-based reasons for taking a watch and wait approach, until a young person can decide for themselves, if there is no medical need – and at dsdfamilies we support many parents who have made the decision to raise their child without surgery. However, by using the term ‘intersex surgeries’, there is little attempt to engage with patient groups for either CAH or hypospadias, who rarely use and frequently reject this terminology. Describing these surgeries as ‘intersex surgeries’ has also allowed hospitals to announce they are stopping intersex surgeries, whilst claiming that hypospadias and CAH have nothing to do with intersex.
Malta is frequently described as the country that has banned intersex surgeries. However, due to the small size of the country, they only banned surgeries that they didn’t perform and excluded hypospadias, resulting in no change to their practice.
This highlights the importance of precise language and clearly defining your population, if you want policy change to be anything more than words.
Why does this matter?
This all comes back to needs – and the needs of the 0.05% being misrepresented or even erased. The most complex and rare cases from the 0.02% are presented as if applicable to the 1.7% or even 4% – but then the lowest need cases from the 4% are presented as if applying to the 0.02%.
For example, in the 2020 paper by Fae Garland and Mitch Travis https://onlinelibrary.wiley.com/doi/10.1111/jols.12223 intersex variations are described as “predominantly benign”. This was also voiced at a talk given by David Griffiths for the Wellcome Trust https://wellcomecollection.org/events/YJPWAhEAACIA7VJE – and highlights the lack of recognition or understanding of the needs of people living with variations of sex development.
As someone born with Complete Androgen Insensitivity Syndrome, there is nothing benign about finding out as a young teen that you were born without a uterus, cervix and upper third of the vagina – and the impact this has on fertility, sexual function and psychological wellbeing. This should be no barrier to a great life – but it is never ‘benign’. I would also ask whether the episodes of life-threatening adrenal crisis associated with CAH are also considered benign – or the heart problems associated with Turner Syndrome? Even infertility is recognised as a disease by the American Medical Association https://www.the-scientist.com/editorial/a-new-view-of-my-own-past-69024 and the grief associated with infertility is well documented.
Presenting intersex as just benign variations, erases the very real medical and psychological needs that should be at the heart of any activism, policy, or research. It also does not allow young people the space to grieve the losses frequently associated with being born with a different body, which is essential if people are to accept their bodies and make a meaningful life. This very much feels like a form of ‘toxic positivity’ – and gives the impression that a bit of flag waving and visibility is all that we need. Being proud of your differences and celebrating diversity can be empowering and hugely rewarding, however, this should be alongside ensuring that medical and psychological needs are also met. Maybe the “benign variation” description is especially loved by policy makers, as it is far cheaper to provide a few flags or to add an I to the end of LGBTQ+, than providing the funding for family, psychological and peer support. Even when the I is added, funding received is limited and less than 1% of overall funding for LGBTI issues. https://lgbtfunders.org/wp-content/uploads/2018/04/2015-2016_Global_Resources_Report.pdf
Increased stigma
Treatment options are also frequently described in the most stigmatising ways, for example in the article linked above by Fae Garland and Mitch Travis, they describe vaginal dilation as “the stretching of the vaginal canal to accommodate a ‘normal’ penis, during childhood either by parents, carers of healthcare professionals”. A similar definition was used in the Intersex Mapping Project Survey, which described dilation as “being made to insert objects into your vagina or front whole” – and a presentation by Celeste Orr during the 2021 Intersex Conference, A Vision for the Future, even presented the idea that mothers were usually the ones to force their children to dilate and were involved in ritualistic and institutionalised sexual abuse of their children.
This is so far removed from anything that is currently happening in the UK and only adds to the stigma associated with being born with a variation of sex development. Describing the worst examples of care and presenting them as happening now, could also significantly impact on the relationship between young people and their healthcare providers.
Many young people with Androgen Insensitivity Syndrome or MRKH, choose to use dilators – and they frequently need significant care, support and sensitivity – and discussing treatment options in this way shows a lack of empathy and understanding, especially when the above talk seems to also suggest that a young person wanting to have a vagina or to have sex with her boyfriend, is all part of a “harmful status quo belief of the medical establishment”. It feels like the very real loss of the young people at the heart of this discussion, are considered as too ‘cis-heteronormative’ to count, especially as it is rare to see similar criticism of dilators when used as part of sex affirming surgeries for trans young people.
Increased risk of surgical interventions
There is also the risk that referring to babies as intersex, especially with the common misunderstanding that this means neither male or female, a third sex or even having both sets of genitals, could result in parents consenting to surgical intervention that may not be needed. This was highlighted in the paper by Annette Smith & Peter Hegarty https://www.tandfonline.com/doi/abs/10.1080/13691058.2020.1788164?journalCode=tchs20 that found that people were more likely to justify clitorectomies, if a baby was described as intersex as compared to describing as female.
This was also discussed by Alice Dreger on her website:
“I learned that, for some of these folks, using the term “disorder of sex development” meant in their minds that you could afford to do less medical intervention on affected children. “Intersex” had a way of feeling totalizing, because it had come to represent an identity (thanks to the intersex rights movement). The people who were uncomfortable with intersex wanted to make it go away in children—they didn’t want their defenceless babies being drafted into a political identity movement. If their children just had a DSD, well, then they just had something that went funny in development, but it didn’t mean their whole bodies and identities were taken over by this thing. It was manageable; they could manage with less medical intervention”http://alicedreger.com/dsd
Loss of privacy
Regardless of how frequently the 1.7% statistic is used, there are only a tiny number of children (far less than the 0.02%) that present at birth with genital difference of a degree that would make sex assignment difficult without further investigations. However, is it fair to label such a tiny number of children as intersex, even if this is only on a social and not a legal basis, as this would result in a significant loss of privacy about their body and medical history. Many parents have to make the difficult balance between ensuring their child understands that nothing about their body is a secret, whilst also respecting that their child has the right to privacy about personal information. Far better for a child to be raised as a boy or girl with a different body, whilst providing the support they need to feel confident about their difference – and whilst keeping an open mind that they may identify in a different way as an adult, and that is also fine.
Funding
The misrepresentation of people born with variations of sex development, has led to significant public confusion, with many people believing that intersex is an identity, possibly a gender identity.
This likely has an impact on funding, which is clearly demonstrated by the difference in funding given to groups that support gender diverse identities, as compared to funding received by groups who support children and young people born with variations of sex development.
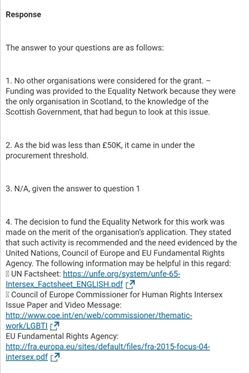
Intersex research based on online surveys that ask people to self-identify as intersex, have also been used to justify giving funding for intersex projects, to groups such as Scottish Equality Network, who have little experience in this area – and have still not produced any project or service that could improve the lives and wellbeing of people with DSD. This is highlighted in the Freedom of Information request detailed below:
Finding accurate information about your body and health needs
One of the most important aspects of the care and support of people born with variations of sex development, is finding accurate and precise information about your body. This allows you to make informed choices about any healthcare options that are offered – and it also helps you to meet other people who share a similar experience. Sadly, intersex terminology now seems to be doing more harm than good. Many young people and even new parents use social media to find sources of information and to develop relationships with other people with similar experiences or medical histories. However, when searching for #intersex on Instagram, there is very little in the way of accurate information and even activist and support groups rarely discuss the condition specific names that are most frequently known and used.
Currently, the top 100 posts for #intersex are as below:
Someone waving a pride flag
Gender creative parenting
Anime trans account talking about finding blue and pink confusing
Bisexual Olympic athlete – assault
Alok Vaid-Menon (non-binary)
Trans memes
Kinky fairy picture
Trans poster
Genderqueer & ceramics with pictures of mild hypospadias
Pride wine glass
Queer sexuality
Queer shop merch
Gay culture
Something about baby yoda being a LGBT icon
LGBT
Trans person being adopted by dad of her BFF
Man in bondage gear waving pride flag
Trans
Drag night
Queer shopping
Pride week in Prague
LGBT
Guardian article about non-binary warrior
Caster Semenya being used to claim no scientific distinction between men and women
LGBT group and article about pope saying god made gay people
Queer community vocab
Someone coming out as intersex and asking to be called hermaphrodite (no diagnosis given)
Kings Lynn Pride
Queer-owned inclusive book box
Trans meme about misgendering
Munroe Bergdorf and 20 thing not to do this year – one of these was don’t erase intersex
LGBT and Romeo and Juliet being gay
LGBT
Trans artist drawing picture of hairy creature with caption “Intersex people shouldn’t feel forced to alter their souls”
LGBT
Post by CEO of cuddlemonstr
Queer t-shirt shops
Someone dancing in pants with hashtags including crossdresser sissy and pantyfetish
Long Beach Trans Pride
Shop queer gear
Queer spaces
Ella festival for queer and non-binary people
Celebrities with tans children
Shop queer gear
EndIntersexSurgery
Seeing Mike Pence swear in a democrat senator while a bisexual woman in a purple wig and zebra print coat holds the bible
Pride hearts knitting
Stop sexualising women and girls for literally just existing
Intersex person
Rainbow crafts
LGBT
LGBTgroup and something about an art teacher being gay
Gender identity and sexualities – pansexual, non-binary
Rainbow family and gay marriage
Folx Sexual Healthcare
The smell of bisexuality in a candle
Queer spaces
Being Asexual
Trans
Rainbow crate book box and Cinderella is dead book
LGBT
Transgender actress joining charmed
Genderless and dissociation
Trans post from tinder
How to be a better trans ally
LGBTQ artwork
Trans and non-binary health and hormones
Queer garden gnomes
Rainbow craft box
Trans parents
Mercy bell cat t-shirt
Gay kissing meme
Trans woman with kids
Trans anime meme
Story about an intersex twin forced to live as a boy and is really a girl inside
How to come out as asexual to friends
Gender elephant
Wearing binders
Cencus
Intersex jusitice is trans justice meme
Possible intersex person
Trans poster
Glitter beards
Gay meme
joke about asexuals
Demi-sexuality
Transcending the binary
LGBT
Queerness and letter to cis-heterosexual parents
Cologne Pride
Trans anime account posting about Caster Semenya also with hashtag trans
Trans memes about on-binary
LGBTQIA+ asexual
Intersexuales Chile
LGBT memes
LGBT memes
Anti trans sports ban
Asking for pronouns
Drag show pride ball
Using emojis for pronouns
Panty fetish man aside (my eyes my eyes) there is possibly a lot of great content in the above posts, however, none of this provides any accurate information that would support young people to find out about their bodily difference or even to develop peer relationships with other young people with a similar diagnosis.
Becoming a meme
When intersex is mentioned on social media, the information is frequently inaccurate and the different bodies of children and young people are described as being ‘neither male or female’ or as third, fourth, fifth or even sixth sexes – and frequent memes are produced that use our bodies, as a way to validate diverse gender identities. Whilst mis-gendering is considered profoundly offensive, the same respect is not given to people with DSD. Even worse, the term has become associated with types of porn and ‘Not Safe For Work (NSFW)’ #intersex posts are becoming increasingly common. This possibly stems from the misunderstanding that intersex means both sets of genitals – and even academics like Anne Fausto-Sterling have subtly presented this narrative, as indicated in the quote below about intersex children (from her book ‘Sexing the Body: Gender Politics and the Construction of Sexuality’):
“It is not so far-fetched to think that some [intersex] can become the most desirable of all possible mates, able to pleasure their partners in a variety of ways.”
Lack of cultural sensitivity
Children with variations of sex development can be born in all geographical areas and to parents from all social, cultural, ethnic, and economic backgrounds – and this includes to socially conservative and religious families. To ensure that as many children as possible get the support they need to grow up feeling positive about their bodies, language and support groups need to be inclusive of diverse communities. Only using intersex terminology and placing the complex issues faced by children with atypical reproductive development, alongside adult sexualities is not always the best way to engage parents of young children. Labelling babies with what some people consider to be a queer or political identity, or even describing intersex as ‘queer bodied’ https://en.wikipedia.org/wiki/Intersex_and_LGBT may confuse and even alienate many parents, preventing children getting vital support. This was discussed by Alice Dreger in the chapter “Twenty Years of Working Towards Intersex Rights”
Misinformation within schools
Presenting intersex as an identity term, is also increasingly being introduced into schools, with little consideration that a child or young person living with a variation of sex development, may not like, use or even know the term applies to them. From discussions with psychologists working in this area, they have stories of young people developing anxiety and depression after realising that the term intersex was being used to describe them – and psychologists will always follow the lead of the young person and will not force language on them, that prevents them from being able to discuss their variation or to share information with friends. A recent example of this was highlighted in the school information provided by Shout Out Ireland https://www.shoutout.ie/blog/attitudes-of-secondary-school-students-in-ireland-towards-intersex-issues who presented ‘intersex’ alongside identities including queer, pansexual and non-binary – with little reference to the very different issues faced by young people.
Misinformation within institutions
Inaccurate information is now frequently shared within organisations, often as part of their Equality and Diversity Training. This has even led to a woman in the UK with Partial Androgen Insensitivity Syndrome, being threatened with disciplinary action at work, after she criticised the information that was shared about intersex – and was left in a difficult position about whether she would need to discuss her medical history.
Failure to prioritise the needs of the most marginalised and vulnerable
In DSD/intersex advocacy, the most vulnerable and marginalised are always going to include babies and children, who have no voice and cannot advocate for themselves. It is essential that parent advocacy should be prioritised if the next generation of children are to grow up and feel confident about their bodily differences.
If intersex terminology is not embraced by the majority of parents, how can any advocacy or activist organisation truly define themselves as inclusive of the needs of all children born with variations of sex development. If receiving peer support depends on parents describing their child as intersex, how inclusive is the support offered?
Hopes for the future.
I want to see a future where ALL children, young people, and adults with variations of sex development, have the family, psychological and peer support they need to live full and meaningful lives. Being born with a different body should not be a barrier to a great life, but support is needed – and this support should not depend on how you choose to identify. We need to recognise that most people use condition specific terms – and that many reject the term intersex and see themselves as someone with a medical condition – and do not feel stigmatised by having a medical condition as this makes them like everyone else in the world.
We need to ensure that the names of our medical conditions are frequently referenced on websites or social media, by any groups working in this area, to ensure that young people and their families can find accurate information about their body and meet others with similar experiences. We need to include language options that allow people to easily share information with their friends and family, at their pace. We need to reclaim the names of our medical conditions #ReclaimOurNames if we are to understand our bodies and make informed choices about our healthcare.
Advocacy, activism and research should try to engage with as many people as possible – to ensure that a diverse range of voices are heard and that people are provided with the support they need, regardless of the terminology they use to describe their body. Possibly the best option is to have support groups with a neutral name, whilst accepting that members may have different thoughts and feelings and may use different terms at different times – and that this it is OK for our opinions to be as diverse as our bodies. Hopefully the future will be more inclusive than adding an I, which far too frequently results in the needs of people with variations of sex development becoming invisible
And for one final thought, maybe the IAD from Intersex Awareness Day, could also stand for Inclusive of ALL people with Different sex development. Maybe not as catchy, but definitely more inclusive.
Being caught up in the gender wars is no fun and I have become increasingly tired of people tagging me into the many ridiculous debates about whether or not sex is binary, bimodal, a spectrum or possibly doesn’t even exist at all. However, I didn’t wade into this debate to argue endlessly about the nature of sex and reproductive development – my aim was always to highlight the similarities between the current discussions of how best to support children with gender dysphoria, and the way that children born with variations of sex development were treated a generation ago. How the ‘born in the wrong body’ narrative has been used to describe both groups of children – and how the ideological belief that emotional distress is best managed by medical and surgical interventions, has been prioritised over open discussion of the evidence.
The longer I have been involved in this debate, the more it has come to remind me of one big mess of emotional dysregulation – and at the heart of this, seems to lie the belief that two things can’t be true at the same time. This has most recently been highlighted by the response of Owen Jones to a mother’s concerns about her child’s gender dysphoria, being treated with medical & surgical interventions.
There seems to be no willingness to listen or to try and understand where someone may be coming from. Instead the most extreme stance is taken, which only leads to an increasingly polarised debate where you are “either with us, or against us”. This helps no-one, especially children and young people experiencing gender dysphoria. It made me think that maybe this whole debate needs a little bit of Dialectical Behavioural Therapy (DBT).
‘Dialectical’ means trying to understand how two ideas that initially seem to be opposing, can be true at the same time – and when considered together can create a new truth. It should be possible to honour the truth on both sides of a conflict – and this does not mean you need to give up your values, but the world is not black and white and there is always more than one way to view a situation.
Dialectics of the gender wars…
Is this a rabbit or a duck? Whilst the Owens of the world may be screaming Rabbit – many others will be screaming Duck. But can this be both a rabbit and a duck?
In a similar way, is it possible for a caring and supportive parent, to want trans people to live without stigma or discrimination, whilst also having concerns that medical and surgical interventions are not the best way to support their child, who is experiencing distress about their gender?
Is it possible for people who genuinely want the best outcome for children and young people experiencing gender dysphoria, to also want open discussion of the evidence and ethical considerations? Does rebranding this as ‘anti-trans’, show a very concrete way of viewing the world and thinking about child development?
In all other areas of paediatrics and child mental health, debates are common. For example, the evidence and ethical considerations of using stimulants for ADHD or SSRIs for depression, are frequently and rigorously discussed. Being critical of their use, does not mean you are a bigot who is ‘phobic’ of children with ADHD or depression. Could it mean that you are not convinced by the evidence, which is often limited in many areas of paediatrics, due to the ethical issues associated with research involving children? I am in favour of the use of both, but only following careful assessment and discussion of risks and benefits – and I encourage open debate and regular reflection on all treatments offered to young people.
The Owens of this world may believe that the only way to support a child with dysphoria, is for medical and surgical interventions to be easily accessible. Whilst on the other side, many believe that no medical or surgical interventions should be available and that psychological interventions should be prioritised. Is it possible that even with seemingly opposite views, both groups are wanting the best outcome for children and young people – and that the truth lies somewhere in the middle?
Maybe the most compassionate and thoughtful approach, would be to prioritise careful assessment, evidence based care and psychological curiosity, whilst acknowledging that for some young people, medical interventions may be in their best interests. However, as with all other presentations to child mental health services, recognising that gender dysphoria is likely to be influenced by biological, psychological and social factors and that not everyone will benefit from a medicalised path, is also vital. Both of these statements, although they initially appear to be opposing, can be true at the same time.
Is it also possible to see affirming or validating in a more nuanced way? This should not mean that we need to agree with everything a young person thinks or feels about themselves, but instead, it means that we should try to understand where they are coming from.
If we really want the best outcome for children and young people – maybe we should all be trying just a little bit harder to understand where people are coming from. Including Mr Jones.
I’ve written a lot about my own experiences of being born with a variation of sex development. However, it is not just my story and it has also had a huge impact on my family, especially my parents. I found it hard to write their story & separate it from my own voice and feelings, but hopefully this catches some of what they experienced. It made my Mum and Sister cry a little – although this included some happy tears, which are the best type of tears and always remind me of Anne of Green Gables.
Happy tears
I now live in a small town just outside London and every year a local family organises a small festival in their very large garden. Everyone dresses up in their most colourful hippy wear and the area fills with flower children and ageing rockers, dancing and drinking to local bands – and it probably comes as close to Woodstock as you can get in a semi-rural Surrey town, that definitely wants to identify as a village.
Last year my Mum, Dad and sister all came along. Although well into their mid-70s, my Dad was dressed in a flowery shirt & psychedelic bandanna and my Mum wore flowers in her hair and had her face painted with glitter. We all danced and laughed, drank far too much prosecco and cheered along to all the bands. As it became dark, I remember looking at my parents as they smiled and clapped along to the music, surrounded by my friends and twinkling fairy lights. I felt so much love for my family and so grateful that we were all here together – and I turned to my sister all gooey eyed and slurred “we need to remember this moment”. The warm summer evening and alcohol may have made me sentimental (there were definitely some happy tears), but it is these moments of shared happiness that are so important for all families – and I think this has been a big part of what has kept us close, even through really difficult times.
A different child
My parents both came of age in the 1960s – and they feel very similar about the 1960s as I do about the 1990s. This was their time and I’ve heard all their stories. My Mum bought everything by The Beatles and wore out her shoes by twisting. My Dad was in a band, who were fairly successful in South Wales and even Tom Jones sang with them. My Dad thought of himself as a bit of a Beach Boy and my Mum shivered on the beach as he tried to catch waves in the middle of winter. However, when they married in 1971, they were both still fairly young and innocent and still living at home with their parents in the houses where they were born.
I was born in 1972, just over a year after they were married. My Mum had a long and difficult labour and I was eventually born by Ventouse, looking like a cone headed alien. She has always blamed this on her teeny tiny size 3-feet – and although there might not be much truth to the idea that pelvic size is mirrored by your feet, her obstetrician later came to see her and told her that they wouldn’t let her suffer like that again.
Although exhausted, she delighted in her little cone-headed baby – and as was normal at this time, she settled down to a couple of weeks stay on the post-natal ward. She enjoyed this time swapping stories and sharing jokes with the other new Mum’s. The first sign that there was anything out of the ordinary, was when she was unexpectedly moved to a private room. She was not given a reason for the move and was told to place all her linen in a bag labelled ‘contaminated’ – and she felt a subtle change in the way the nursing staff were treating her. Already exhausted and vulnerable from the birth, suddenly finding herself in a room on her own, led to increasing anxiety and the sense that there was something terribly wrong. My sunny natured always ‘glass half full’ Dad, tried to reassure her. However, she continued to worry, even after she was allowed home, especially as she was the only new Mum to be given a follow up appointment back at the hospital.
She also sensed something when the midwife visited her at home – and she asked many times if there was anything wrong or why she had been given another appointment back at the hospital. She was not given a clear answer and was just advised that it was all routine. However, at the follow up appointment, the doctor’s first question was “are you planning to have any more children?”. She tried to express that she had only just given birth and hadn’t given this any thought – and he replied that maybe this was something she would need to think about. This led to her feeling increasingly panicked and again she asked if there was anything wrong or something they weren’t telling her, but he dismissed her worries, although gave her another appointment to see a Professor of Paediatrics.
When I spoke to my Mum about this recently, you could see that she still felt upset about this experience, even stating “I hated that doctor”. He also later turned out to be a parent of another child at my school – and every time she saw him, she felt scared that he recognised her and that he knew this secret information about me.
A few months later, we had the appointment with the Professor, who my parents remembered as a kind and warm man. He explained that when I was born they noticed I had hernias – and following this they checked my chromosomes and found out I had XY chromosomes. My parents were not given any name or much further information, but he explained that I should never find out and that they shouldn’t tell other people. They were told they would repair my hernias after I was 2-years-old, unless there was any indication that this needed to be done more urgently. When I was a bit older, they would tell me a story to explain why I couldn’t have children and didn’t have periods – and that in the future there would likely be womb and ovary transplants. My parents asked if there was anyone else, but they were told that this was something incredibly rare and it was unlikely that there was anyone else in the area.
Just before my first Christmas, my Mum was at home alone, whilst my Dad had gone out to watch the Football (he is still a huge Cardiff City Supporter). I started crying and although my Mum tried to soothe me, nothing worked and the crying turned to screaming. When my Dad returned home, they took me straight to A&E and I was immediately admitted and underwent an emergency hernia repair. When I came out of surgery, the nurse looking after me on the ward stated, “it’s a good thing I put her in a blue Babygro”. The distress caused by this comment, especially following the rush to hospital and emergency surgery on her three-month-old baby, led to my Mum fainting. My Dad caught her before hitting the floor and she wasn’t physically hurt. However, emotionally she was also falling – and there was no safety net or support available to catch her as she plummeted into the unknown of what it meant to have a child with a variation in sex development. This wasn’t an experience she could laugh and joke about with the other new Mum’s. This was something more than whether I was sleeping at night or teething – this was something they had been told should stay secret, even from close family and friends. Almost every interaction with health professionals, had only added to their feelings of shame and isolation – as well as making them believe that they must never let me find out. My future wellbeing was dependent on their silence.
We continued to see the Professor over the next few years and my Mum felt so grateful to him for just being kind, that she even gave him my cot to give to his new grandchild. Their circle of support was so small, that he was one of the only people that they could talk to – and they didn’t question any of the advice or information that he gave them and they saw him as the only person who could help. My parents were introduced to his registrar, who later took over my care when the Professor retired. Throughout my childhood and even into my adolescence, he was their only source of information and reassurance.
I recently spoke to my Mum about this time and she described living in a constant state of fear and anxiety, questioning my behaviour, appearance and quirks and worrying about what this meant for my future. She commented that she often felt like she was ‘walking around like a zombie’, going through the motions of parenting, but never fully present. She had been told that I would likely be tall and she worried that even as a young child, I was taller than many of my peers. She pictured me being 6ft4, even though she was only 5ft2 and my Dad barely 5ft7 – and she thought I would tower over my sister. The reality was somewhere in the middle – and although I am on the tall side, I am not quite 5ft9 and even my sister is taller than my Dad.
My Mum also described once taking me to see my GP for a sore throat, likely after shouting far too much on a week away with my school. The GP stated, “maybe it is to do with what she has got, it is probably her voice breaking”. Although my total insensitivity to androgens has resulted in my voice always being on the ultrasonic side of normal, this comment devastated my Mum. Not just from the fear of my voice unexpectedly breaking, but because of the callousness of the remark, with no sensitivity to how this could make her feel or how alone she felt. It was months until my next hospital appointment and my Dad was the only person she could share this with.
When I was 14, I was given the devastating and fictional story of needing to have my pre-cancerous ovaries removed – and I was also told that I didn’t need to tell anyone. The lies and secrecy became an increasingly oppressive silence that impacted on all areas of our family life. I felt deep shame about my body and with no words to express this, it turned inwards and to hatred of my appearance. I became obsessed with the shape of my nose, wrinkles on my youthful forehead and fears that my eyelashes were falling out. My Mum recalled me becoming hysterical after finding another eyelash on my cheek – and I subsequently saw my GP and was referred to a counsellor. My parents were also seen by a therapist at the same unit. But what good is talking therapy, when I didn’t know the truth and my parents were too afraid to even tell the therapist the truth – and we were only able to superficially discuss our worries.
Outside of my family, I also appeared to be a healthy and well-adjusted young person, doing well at school and with a good friendship group. I was articulate and could play the part of a normal happy teenager. However, at home I had frequent episodes of distress. I would cry because I was so afraid that I would never be loved – or because my physical appearance was not perfect enough to make up for what I felt that I lacked. It is only years later that I would really understand how difficult it is to see your child in pain and the impact this also had on my parents. When I was finally told the truth about my diagnosis (see previous blog post https://differently-normal.com/2020/08/03/tale-of-a-good-gp/ ), they also had to accept my anger – as well as the shame of feeling that they had done everything wrong.
Moving forward with the truth
After I was given the truth about my diagnosis, I contacted the AIS support group and arranged to attend a support group meeting. My parents came with me and at the beginning I think they felt that they were coming to support me – and although this was a really rewarding experience for me, I think it was even more important for my parents. For the first time they could meet other parents of children with different sex development – and they were able to share their similar experiences and stories. They found support and understanding amongst other parents who had made similar decisions – and had also clung to the advice they were given, not questioning & just feeling desperate for any guidance. They looked around the room and saw other young people like me – and even though there was a lot of hurt and pain, we were not broken. They could see that there was no reason why any of us should feel ashamed – and that we were all imperfectly perfect people, starting to find our own voice.
Family relationships are rarely simple – and although we were able to take the first steps to rebuilding our relationship, we continued to have conversations that were incredibly painful for us all and the scars are still there. But we are also very much involved in each other’s lives. As a family we are noisy and squabble furiously, but there is also lots of love, warmth and fun.
My life is now good, I have a job that I love and I’m married with the most amazing son through adoption. Although I can recognise the mistakes my parents made in keeping the truth from me for so long, I can also recognise that their love and support, even during the most difficult of times, is a big part of why my life is now good. Even though they were made to feel that my diagnosis was something shameful and should always be kept secret, I was always loved. There was always someone to pick me up when I cried, my Dad would play with me for hours (and only now as a parent do I understand the patience needed to play schools for hours) and my Mum would sing me silly songs, which is a habit that I have now inherited with my son. My childhood was full of stories, magic and imagination and all of this gave me resilience.
The family as a therapeutic resource
I now work with children and families, possibly because these experiences influenced and directed my career choices. When I see young people, I am always aware that it can be incredibly difficult to really make a difference to their life, if support is not also offered to the whole family. I have seen the importance of family therapy, for helping parents draw on their strengths and work together to support their child.
I do wonder what difference it would have made to my life, if my parents had been offered support. If they had been able to meet other parents and had been encouraged to talk to people they trusted. If someone had given them the words to talk to me about my body – and instead of silence, I could have been helped to understand that although I was different, this was no barrier to having a good life. I could have been supported to understand that I should not feel ashamed and that there was nothing about me that needed to be kept hidden.
Even today it is difficult for parents of children with different sex development, to get the support they need. In the UK, it is now advised that children should be told the truth about their bodies, but parents are not always given the words and narratives to explain things in an age appropriate way. It is also advised that specialist psychological support should be available, but this is rarely adequately funded. Far too frequently, parents are still depending on a yearly appointment with a doctor or surgeon, for all their information and advice – and there is very little support for the other 364-days of the years. This leaves little time to discuss the many issues a family might face or to have the difficult conversations that are sometimes needed. I worry that this can lead to simple solutions being given for complex problems, possibly as the time to just sit with a parent’s distress, is not available.
Most parents love their children and this is hugely important for helping children grow up to be confident and resilient. However, love is not enough and parents also need support – and I do wonder if family support could make the biggest difference to the wellbeing of children with different sex development. With the right support and funding, the child’s family can become the most powerful resource, for developing an environment where a child can grow up without stigma and shame. This is where support for groups like www.dsdfamilies.org could make a huge difference to the wellbeing of families facing these complex issues, helping them to understand that surgery and silence is not the only option.
I decided to apply to medical school when I was 30. This was a decision that I made overnight after reading about the new Graduate Entry course in a copy of the Evening Standard that had been left in my shared house. “I can do that”, I thought – “it will be easy, they need loads of doctors.” The reality was not quite as simple and I suddenly found myself jumping through the various hoops of entrance exams, applications, actual medical school, more exams, junior doctor years, more and more exams – and although it is now almost 17-years since I first read that article, I am still in training (although almost there).
I still sometimes wonder why I put myself through all this, especially later in life than the average medic. As for many bright young kids who like science, medicine was suggested to me throughout school – but it was always a very definite NO! My experience of doctors had not been good. My childhood doctor who had been kind enough, had given me devastating news about my body, all wrapped up in a cloak of secrecy and then seemed to just disappear. My transition to adult services, resulted in my questions about the effects of HRT on my body, being dismissed as “Ah, but it is a good for girls to have large breasts”. Medicine was definitely not for me.
I started university for the first time, in Brighton in the early 90s – and was subsequently referred to a hospital in London. However, I was again not provided with any more support to understand my body. The information given to me by the doctors I saw, continued to be inaccurate or even completely untrue. For most of my university days, I was able to keep the shame I felt about my body locked away and I had a good time. I made some great friends that I am still close to today – and I loved our shared house with our very own disco room. I drank far too much and would wear my best clubbing clothes to exams, as after exams there was always a ‘night out’. However, the hurt was there, hidden inside and always seemed to surface on the train up to London for my hospital appointments. I was usually quietly sobbing by the time I reached Victoria and I would continue to cry on the Tube and throughout my appointment. This made it even more difficult to express how confused I was and how many fears I had about my body. At one appointment, I begged for surgery that would somehow give me a vagina that was the ‘right length’. I was given the usual waffle about waiting until you meet a nice understanding ‘husband’ – and I think I sobbed “but I just want to have sex with anyone, whenever I want – just like everyone else”. This did not go down well and I was told curtly that she didn’t operate so that young people could just ‘sleep around’. This made me cry even harder and she told me that it seemed like I had mental health issues and maybe I should get support with that. I would continue to cry uncontrollably on the train on the way home, only stopping when I finally reached Brighton. My distress would then once again be locked away and I would go back to my shared house to drink wine (usually Bulgaria’s finest or Le Piat D’or, if we were feeling posh).
After finishing university, I stayed living in Brighton, so that I could continue to live with my friends. We all had quite silly temporary jobs, so that we could continue to fund our social life and mine mostly involved taking out staples for the ridiculously named ‘Uplift Team’ of an insurance company (someone on the other side of the table, restapled the documents once they were ‘microfiched’). Although for the most part, I was still superficially living a great life, the days of despair when I just wanted to take to my bed and cry, were starting to become more frequent. During this time, I registered with a new GP practice. My GP was a young woman, probably in her early 30s and she was kind, thoughtful and really listened to me. I was able to share with her how desperately unhappy I felt at times – as well as how confused I was about the information I had been given about my body.
She arranged for me to see a psychologist and so off I went into deepest darkest Hove, which at the time seemed a great distance. Every week I would talk to him about what had happened to me, the confusion that I felt as well as the periods where I felt so unhappy. I would also talk about the very ordinary parts of my life, eating dinner with friends, nights out and days at the beach. After talking to him for a few months he recommended that it might be helpful for me to have a proper look at my medical notes – and that he would talk to my GP about arranging a time for this to happen.
This was all happening during the summer of 1996, the Spice Girls had just released Wannabe and everyone had gone Football Crazy with Euro ’96. My sister was also graduating from University in London and so I went up to meet her and my parents for a celebratory meal in Chinatown. After the meal and as we were walking back to the Tube, I casually mentioned to my parents that I was due to see my GP the next day to go through all my medical notes. I had no idea at the time, but my parents were terrified by this, although managed to ask me for the name of my GP before I headed home.
The next day was a beautiful sunny Brighton day and I took my favourite back route to the surgery. This passed along (as I liked to call it) the alley of fragrant stones and then through the houses with the little flashes of sea as you passed by each road – and then down towards the Pavilion.
I felt light and almost skipped into the surgery, I had no fear and was not expecting to find out anything exceptional, possibly just a little clarity over my body and what had happened to me.
In her large sunny room, my GP sat alongside me with my medical notes in front of her. She started to tell me about how babies develop in the womb. She told me that for around the first two months, the embryo has the potential structures to develop as either male or female. However, if you have XY chromosomes, this will lead to the development of testes, which will then lead to the production of testosterone and the development of the normal male reproductive system. She explained that I had XY chromosomes and that as an embryo I had developed testes. However, as my body is completely insensitive to androgens, I was unable to respond to the testosterone I produced and my body therefore did not develop the normal male structures and instead I developed along the female route – and at birth I would have been indistinguishable from any other girl, although without a uterus or top part of the vagina.
“Wow”, I thought “this makes sense and there is a name”
Androgen Insensitivity Syndrome
I did not feel upset or traumatised by this information – it just made sense and was the first piece of the puzzle that would lead to me putting myself back together as a whole person.
“Wait till I tell my parents”, I stated. She looked at me kindly and replied “they already know – they have been calling here all day and begging me not to tell you and they are desperate to talk to you.”
This was the information that was really shocking to me. Everyone had known. My medical notes were littered with the phrases ‘she does not know the truth’, ‘she should never know the truth’.
My GP explained that my parents had been told that my diagnosis of Androgen Insensitivity Syndrome and my XY chromosomes, should be kept a secret. They were told that this information would likely be too traumatising for me to hear and would lead to significant mental health problems. They had tried to do what they had thought was best, what the doctors had all told them was in my best interests.
I could see my GP was troubled – and she explained that she really hoped she had done the right thing by telling me, as everywhere in my notes it had stated that I shouldn’t know the truth. She felt that this was wrong and that the confusion about my body was causing me distress. However, one of the reasons she had wanted me to see a psychologist, was to get a second opinion, to ensure that I would be able to cope with this information. He confirmed that although I was confused and distressed, I was bright and mentally resilient and deserved the truth about my body. My GP gave me information and the telephone number of a support group for people with Androgen Insensitivity Syndrome (AIS) and told me to come back and see her again soon, if I had any questions.
I left the surgery in shock, not at the new information I had learned about myself, but about the years of secrecy and the lies that I had been told. My pre-cancerous ovaries were not ovaries at all and were not pre-cancerous. All the many doctors I had seen had all known and had continued to lie about my body, even when I asked them directly if there was anything else. I had even previously begged my parents to tell me if they knew anything else, but they had always claimed that they knew nothing more than the doctors had told me.
I couldn’t yet face talking to my parents, what would I say to them – and how would they be able to explain? I walked to a phone box and called my house and arranged to meet my friend in a pub on the way home. I ordered a double whisky as a way to try and absorb the shock – and I sat down at a table to wait for my friend. Before she came, someone approached me and gave me a small bunch of flowers. I have no memory of who they were or what they looked like, although I remember them telling me that they had never seen anyone look like me before and they just wanted to do something to help me feel better. I think the shock and pain must have been clearly etched on my face, almost like the years of shame and secrecy were finally becoming unbound and making themselves seen. The whisky helped and after a short time my friend joined me and I was able to tell her all the truth – and for the first time, this was the real truth. She listened and we drank more whisky until I felt able to face the walk home.
My parents had also been calling my house, desperate to talk to me and desperate to explain. I spoke to them briefly and we arranged for them to come and see me the next day. Everything was still too raw for me to be able to understand what they had also been through. It would take me some years before I was really able to put myself in their position and realise that even though they had made mistakes, they had always wanted the best for me. However, maybe these initial honest conversations, were the first steps towards rebuilding trust and repairing our relationship.
I don’t think I went back to see my GP and after talking to my friend and seeing my parents, I put my new knowledge and diagnosis back in a box and spent the next few months in a whirl of gin and tonics after work, clubbing and even easy listening discos (they really were a thing in the 90s). The piece of paper with the telephone number for the AIS support group, remained folded up in my address book (also a big thing in the 90s) – and it was only a year later that I was finally ready to dial those numbers and try to make contact with other people like me.
I still think about my GP and how brave she was to dismiss the multiple statements of ‘she should never know’ that were written in my notes – and how she was able to really consider what was in my best interests. I often hear people saying that GPs aren’t experts, which is true, they are not experts in specific medical conditions. However, they are experts in their patients – and often understand their patients in a way that no other speciality is able to achieve. Although, after medical school, I eventually took a different path and did not specialise in general practice – it was a GP that inspired me to take those very first steps. It was a GP that made me see the difference a good doctor could make to someone’s life.
I would like to say a big thank you to this very caring and brave GP, as the truth was the first step towards rebuilding myself and accepting my different body. I would also like to thank all the other GPs who support and advocate for their patients – what you do is not always appreciated, but it is so important.
“We moved on the Tuesday before Labour Day. I knew what the weather was like the second I got up, I knew because I caught my mother sniffing under her arms. She always does that when it’s hot and humid to make sure her deodorant’s working. I don’t use deodorant yet. I don’t think people start to smell bad until they’re at least twelve. So I’ve still got a few months to go.“
This is the start of Judy Bloom’s wonderful ‘Are you there God? It’s me, Margaret’ – and as a woman with Complete Androgen Insensitivity Syndrome, I am now coming up almost 48 and still have armpits that will not tell you if it is hot and humid, which most of the time is a pretty good thing.
Like most other girls who grew up in the 70s and 80s, I loved Judy Bloom. We all shared the books in school and we were all desperate to read ‘that bit’ in Forever – and I will always be unable to say the name ‘Ralph’ with a straight face. My younger sister was bought her copy of ‘Are You There God?’ when she was about 11 – and she was even inspired to start her own secret club based on the book. Every week a group of her friends would meet in our garage to do some bra pinging, before heading off with their notebooks for an afternoon of boy spotting. This mostly involved writing down the names of the boys who lived on our road and then being chased home after accidently giving someone a dirty look or shouting, “Builder’s Bum” at our creepy neighbour. Like the four PTSs (Pre-Teen Sensations), they called themselves the PPBWs (Panty Pad Bra Wearers) and would do a few rounds of “I must, I must, I must increase my Bust” at the start and end of every meeting.
I’m 2-years older than my sister and would have been around 13 when I read ‘Are You There God?’ and at that time I was still expecting puberty to progress in the normal way. But it didn’t – and there were no stories to guide me through my adolescence and into adulthood. Margaret prayed that she would be ‘normal’ and the book is a wonderful way to relieve the many fears about the normal changes that happen to bodies at puberty. It details the excruciatingly painful embarrassment of feeling that your body is out of your control and the importance of being given accurate information about your body. But what if your body is different – and things just don’t happen as you expect? Where was my story and all the information that I needed to know? If I was Margaret, what questions would I have been asking?
Where is my hair and other wonderings?
My best friend when I was 11 was ‘the coolest girl in the school’. She had an older sister and always had that little bit more knowledge than the rest of us. She was the first to have a ‘Frankie Says Relax’ T-shirt, taught us all a dance routine to Toyah’s ‘Street Creature’ and decided that we were going to have a Mods versus Rockers showdown, although I don’t think any of us really knew what Mods or Rockers were, but this didn’t stop us calling the boys Rockers and getting almost every girl in the school marching around the playground shouting “Who do we want, we want Mods, when do we want them? Now”.
Everything seems to change as you come to the end of primary school. We were less interested in skipping and playing bulldogs and more interested in sitting in the cloakroom and chatting. We became aware of the first signs of puberty and gossiped about who was wearing a bra. My friend decided that it would be a great idea to take a poll and ask everyone in our year if they were “growing hair down there”. Although there were lots of shocked faces at the question, most people answered and in nearly all cases the first signs of puberty were doing their thing. Why I was follicly challenged in my nether regions, did not cause me any significant concern at this time. Although I did become more self-conscious as I grew older and still nothing changed – and there continued to be a total lack of hairs springing out of my bikini line. However, I smiled along as my friends talked about shaving under their arms or the pain of waxing, even though the razor remained an object of mystery to me. Amongst all my many hospital appointments, pubic hair or underarm hair was never mentioned and therefore became another part of my body that I just didn’t understand.
I always felt that little bit of shame about my lack of body hair, especially as this has become another area of debate and my naturally hairless state has become associated with pornography. Even Caitlin Moran in ‘How To Be a Woman’ declared a Brazilian to be “a ruinously high maintenance, itchy, cold looking child’s fanny” and stated
“In fact, in recent years I have become more and more didactic about pubic hair – to the point where I now believe that there are only four things a grown, modern woman should have: a pair of yellow shoes (they unexpectedly go with everything) a friend who will come and post bail at 4am, a failsafe pie recipe, and a proper muff. A big, hairy minge. A lovely furry moof that looks – when she sits naked – as if she has a marmoset sitting in her lap”.
When reading this (and I did otherwise love the book), I really wanted to shout out “I would if I could Caitlin, but I can’t”. I’m also a failure on the yellow shoes and pie making, but at least I could do something about that. But no amount of watering or follicle stimulating products will allow me to sprout a proper furry muff. My Brazilian is all au naturel.
One of the great things about finally being given the truth about my diagnosis, was discovering that my lack of body hair was all down to my total lack of sensitivity to androgens. Without a good old dose of testosterone, you will always be fuzz free and never in need of any of the millions of hair removal products that women are told they desperately need. Maybe my perfect bikini line and silky-smooth armpits, make me look as high maintenance as any Love Island Contestant, but I really do laugh in the face of Veet – ha ha!
Along with my lack of body hair, my insensitivity to androgens also means that I have wonderfully fragrant armpits. They just refuse to pong, regardless of how long I ignore them. I could live in a Sauna without soap and still emerge smelling as fresh and lovely as a summer breeze. As a teen, I religiously applied my deodorant to ward off the smells and to feel ‘just like everyone else’, but it is now a good 20-years since I last deodorised and that has to be a bit of a bonus. According to the many deodorant adverts, I am free to wave my arms in the air like I just don’t care, as much as I like – lucky me!
I have also never had a spot, freckles galore, but never a good old squeezable blackhead. This is also probably a good thing, although from watching Dr Pimple videos on YouTube, it does look as if there is something wonderfully satisfying about the perfect pimple squeeze. But along with periods and pubic hair, this is not an experience that I will ever be able to share – and again, this was something that was never discussed with me.
Unit 7
I am not sure if all schools in the 80s followed a similar curriculum, but our sex education came at the end of Form 1 (first year of secondary school, now Year 7). It was the seventh science topic, usually taught in the summer term – and there was much excitement in the weeks before, as it was going to be discussing S E X. As this was all pre-internet, this was how we got most of the information about our bodies and what to expect during puberty. The reality was nowhere near as exciting and mostly involved labelling pictures of male and female reproductive system, although hearing your teacher say ‘ejaculation’ will always be funny when you are 12 (and sadly even when in your 40s). We also spent time in the school library, looking at books about puberty and wondering where we were on the Tanner Stages. During that first year of secondary school, there was also lots of talk about whether you had started your periods, although I don’t remember any excited phone calls of “I got it, I got it” as in ‘Are You There God?’. This talk did become less common as we got older, as it was just accepted that everyone had started and it was therefore no longer something to gossip over – and from discussions with friends, had more frequently become something to endure.
Although I didn’t realise this at the time, there were no pictures in Unit 7 or any of the books on puberty, that described my own anatomy – and I don’t think I’ve ever seen an anatomical drawing detailing the internal anatomy of someone with CAIS. Even when I was told at 14 that my ovaries needed to be removed due to being pre-cancerous (see previous blog – https://differently-normal.com/2020/07/07/girl-in-the-snow/) and was given this as a reason for not having periods, Unit 7 had not prepared me for being able to ask “BUT WHERE IS MY UTERUS”. I feel slightly ashamed of myself now, that even as a bright and intelligent teenager, who was especially good at science – I did not manage to put two and two together and realise that no periods might have something to do with that mysterious uterus that I had labelled with so much care. It was only in my early 20s that I finally found out about the missing uterus and that my doctors had somehow ‘forgotten’ to tell me about this. How this is so easily forgotten, I really don’t know? It is a uterus and something that is really quite important, especially to teenage girls wanting to understand their body. It is not like forgetting to eat your lunch or losing your keys, it is a uterus. I may have to shout uterus a few more times to really hammer this home – UTERUS UTERUS UTERUS!
All of this comes back to the secrecy that surrounded my body – and without accurate information and the opportunity to ask questions, the confusion can very easily lead to silence and shame. Even when I was finally given my diagnosis, the words used to describe my body were frequently dehumanising and stigmatising. My height and long legs were referred to as ‘eunochoid propotions’ and my fairly normal breast development was described as ‘frequently voluptuous’, which is a word that should be banned along with moist and buttons (I also have button phobia, which really is a thing). Even my nipples were horribly described as ‘immature in appearance’, which basically means slightly paler in colour than the average nipple. And who actually writes this stuff – and who do they write it for? If all doctors learn is that women with CAIS are voluptuous eunochoids with immature nipples, how will they ever be able to meet our needs and support us to feel good about our bodies. On the other side, are the discussions of my body being a third, fourth or even fifth sex (thanks Fausto Sterling, I know it was supposed to be ‘tongue in cheek’, but really, was this in our best interests? https://www.researchgate.net/publication/239657377_The_Five_Sexes_Why_Male_and_Female_are_not_Enough ).
All of this has the effect of making you feel like a number of slightly freakish body parts somehow melded together – and that our bodies should be hidden, fetishised or deconstructed. Caught somewhere between sounding like a Love Island Contestant and a Circus Curiosity. These approaches do not centre the needs of people born with intersex variations, as they do not allow us to define ourselves and receive accurate and honest information about our bodies. They do not allow us the opportunity to tell our own stories, in our own words.
My Margaret Moments.
I was finally given accurate information about my diagnosis and my body when I was in my mid-20s. This gave me the opportunity to meet other girls and women like me – and in my late 20s, I attended a number of support groups meetings for women with AIS. Through these meetings I met my very own PTSs, both Pre and Post Teen Sensations, all with different bodies & similar experiences to my own.
I have a great memory of a very drunken evening spent with other androgen insensitive women and terrifying our waiter by demanding he looked at our lovely hairless armpits. We even spent a day designing our very own merkins (genital toupees), wonderfully furry affairs that would even have made Caitlin Moran proud.
Maybe this was my very own Margaret moment – even though I was in my 20s, flashing my armpits and wearing a giant furry muff over my jeans, was my own version of “I must, I must, I must increase my bust”. Women with different bodies, brought together and feeling a sense of belonging from their shared experiences. All of us having experienced a puberty that was anything but expected.
And if you are still there God? We need more of this.
Whilst living with friends in London in the late 90s and thinking about what I was going to do with the rest of my life, I listened to a lot of Belle and Sebastian. I especially loved the song Fox in the Snow and thought of myself as like the ‘Girl in the Snow’.
Girl in the snow, where do you go To find someone that will do? To tell someone all the truth before it kills you They listen to your crazy laugh Before you hang a right And disappear from sight What do they know anyway? You’ll read it in a book What do they know anyway? You’ll read it in a book tonight
There was a secret about me that did not yet have a name, although I knew that my body was different to the bodies of my friends, who had launched into the magic and misery of first loves and young adult relationships. Although always first on the dance floor and often last standing (and usually still drinking) at the end of the night, I watched from the sidelines as my peers seemed to move effortlessly into the next stages of their lives.
I first found out that there was something different about my body when I was just 14. I had spent the previous few months recovering from the surgery I had been told was needed to repair hernias. I had felt almost excited before the surgery, as I was missing school and had been told it would be simple and easy and nothing to fear. My Dad’s new job also came with BUPA cover and the hospital seemed more like a hotel, even having a TV in my room. The reality was very different. The pain was unexpected and terrifying – and although I almost looked forward to the injections of morphine, they made me hallucinate and horribly constipated. The TV became something to dread as even Esther Rantzen on That’s Life made me laugh and laughing is not easy after surgery – and I had to ban my sister from visiting as just one look at her made me painfully giggle. Things were initially better once back at home, although the stitches came apart and I developed an infection and needed daily dressings and salt baths. It was after this summer lost in daytime TV (I was watching Neighbours long before anyone else), that I found myself sitting in my childhood doctor’s office with my parents.
“I expect you are wondering why you haven’t started your periods” my doctor asked.
I felt like I almost had a premonition of what he was going to say next, as I didn’t feel shocked as his life changing words washed over me. “Hernias… damaged ovaries… pre-cancerous… needed to be removed… can’t have children”. It seemed as if the appointment lasted for only minutes and then we were back outside again and I don’t remember crying. Maybe I should have noticed that my parents were also not crying, but I just accepted that this information was as new to them as it was to me.
Afterwards we went for a drive – it was one of my favourite drives, into the mountains where you can see the lights of the city and down into the valley below to see the house where I was born. I had heard all the stories about myself as a baby, the time I posted all the letters back out of the letterbox and my parent’s bills went floating up the hill – and the time I picked all of the beautiful flowers that had been planted in our garden and proudly stated “floo floos”. I had heard about how they would place me on the mat in front of them and marvel that I was theirs, this little person that they had made and loved more than anything. But I never heard the stories of how they had sat in that house feeling terrified and alone, knowing that there was something about their new daughter that they could not share with anyone. A secret they had been told to keep, even from me.
On the way home, my parents told me that it was OK, nobody needed to know, I could tell anyone who asked that I had started my periods over the summer, nobody needed to know the truth. Nobody needed to know.
The next day everything seemed back to normal. It was still summer and we sat in the garden, watched TV, argued as families sometimes argue – and a few weeks later I was back at school and celebrating my fifteenth birthday. Nobody mentioned the appointment or spoke about what I had been told – nobody asked if I was feeling OK. I just carried on the same as before, except that now I had this secret.
A few months later I saw my GP for something unrelated. I remember him as a big self-assured man, who was likely approaching retirement and prioritised competence over his bedside manner. “You’ve had the surgery then?” he asked. As I nodded he added “and you’ll be needing another surgery before you will be able to have sex”. I was only 15 and did not know how to respond to this or even what questions to ask, so just remained silent. When back at home, I tried to ask my parents what he had meant, but again I was 15 and did not have the language to know the right thing to say. They told me it was possible that something about this had been mentioned, but that they had been told that things might be difficult at first, but it should be OK if I meet a nice husband.
I had again been given some words about my body, but not the voice to express them or the opportunity to question them. I buried the words along with the shame I felt and didn’t say them out loud again for the next few years. It wasn’t even the real truth that remained buried and unspoken, but the lies I had been told about unexpectedly finding pre-cancerous ovaries that needed to be removed.
I was given hormone replacement tablets to take every day, with a glass of orange juice at breakfast. The HRT changed my body dramatically from a natural B cup pre surgery, to a G cup within a couple of months. My childhood doctor had left and when I tried to share my worries about my changing body with my new hospital specialist, he told me that I should be pleased as it was good for girls to have large breasts. I did not go back to see him again and I don’t think anyone really noticed that I was lost to follow up. I could get the HRT on repeat prescription and there was no other support that they offered and they no longer even needed to measure me or marvel at my different body. In their view I had been fixed – but inside where my feelings of shame were buried, I felt broken.
I was 15 in 1987, with teen films and first love everywhere, from Dirty Dancing and Pretty in Pink – even Scott and Charlene in Neighbours. There was always some problem to overcome, being from the wrong side of town or being unable to dance (carrying watermelons), but nobody had a secret like mine. In all the teenage fears of first love, first sex, first heartbreak, even fear of pregnancy – there was never a fear of your body being unable to do any of this at all. This felt like my secret alone – and how could I tell anyone the truth, when I didn’t even know the full truth myself. But there is only so long that you can keep anything buried. Shame is corrosive and it will always find a way to seep out into other areas of your life and colour the way you see everything, becoming part of the many ways you can find to hate yourself.
The lies I was told did not protect me, they did not protect my family – they left us without the language and voice to even find support. They left us isolated and alone. My parents never met any other parents experiencing something similar – even being told that it was very unlikely that they would meet anyone else as I was just too rare. Even today in our modern NHS, where communication skills and patient voices are increasingly prioritised, I still hear similar stories of young people and their families facing these issues alone, with no specialist nurses or psychologists to help them navigate the many difficult decisions they are faced with. Far too frequently they are not signposted to support groups such as www.dsdfamilies.org and young people grow up with the same feelings of shame, never meeting other young people with similar experiences.
Parents should not be left to support their children alone, without being offered the psychological and peer support that will help them find the words to tell their children that it is OK to be different and that they can feel proud of their bodies. We need coming of age stories for young people with different bodies, so we know that we can be loved and accepted as we are. We need to know that our bodies are not shameful and that we can share as much or as little as we want about ourselves. We need to know that we are not a secret. Just like the Girl in the Snow sang about needing to tell someone the truth before it killed her, I was only ever able to mend myself once I knew my truth and was able to share this and feel accepted.
Throughout my childhood I had regular hospital appointments. This was at our very big but local hospital and it would usually involve missing a day of school, which always seemed to result in missing some major school gossip as something exciting always seemed to happen on the day that I was away. As many things do in childhood, the appointment took on a routine of its own. There was always the driving around and around the car park looking for a space, followed by walking along the endless corridors and trying to guess whether the door in front needed to be pushed or pulled – and then finally realising that you could work this out by the shape of the handle. The murals on the walls were the first sign that you were entering the world of paediatrics and we would eventually find the clinic and sit and wait to be seen.
The first thing that always happened was a weight and height check by the nurse, who was also a Mum from my swimming club. It was only years later that I realised how stressful this was for my Mum – and how worried she was that someone she knew, had access to my medical records. The fear that someone else knew that I had Complete Androgen Insensitivity Syndrome. Following this, there would always be the wait to see the doctor, which seemed to take hours, but eventually my name would be called.
The meeting with the doctor would usually start with a discussion of my growth chart and how tall I was, usually hovering just above the 90th centile and I liked seeing how my height followed the curve. Sometimes I would also be sent for an X-ray of my wrist to try and work out an estimate of my final adult height. I would usually be taken into the clinical area to be examined, which usually involved (in medical language) inspecting and palpating the area around my inguinal canal – or (in non-medical language), a genital inspection and feeling under the top of my underwear and along my groin area. I had no idea why any of this was being done. I was told that I had hernias, which always seemed slightly strange and something to feel ashamed of, although I didn’t really know why. I remember asking about hernias and being told that it was a bit of muscle that can poke out through your stomach (definitely non-medical language) and that this had happened to a friend of my Granddad. I remember feeling confused about this as I was young and could see no muscle poking through anything. Towards the end of the appointment, I would be asked to sit outside in the waiting room. This always seemed like an even longer wait and I would wonder what they were talking about without me. What was I not allowed to hear? Afterwards, they would tell me that they were talking about how well I was doing or talking about ‘the surgery’ that was looming in my future. I was a child and just accepted this – it was all my normal.
I never felt traumatised by these appointments, they were just one of the many strange events of childhood that become your normal. Nobody was unkind to me and nothing was painful – I was measured and stared at and inspected, but didn’t think there was anything especially unusual about me. I just accepted that this must be what happens to anyone who needs ‘a surgery’ sometime in the future. It was filed alongside other routine childhood moments like going to the dentist or even having my hair cut. It is only looking back later that I realised my normal was not normal at all, but all part of the many layers of shame and stigma that made the reality of my body ‘something that should not be named’.
I’ve met other people who share my history of being born with different sex development and having a childhood punctuated by hospital visits, investigations and examinations. I later even heard people tell stories of photographs being taken of them when they were children or young adults. These photos were taken of them without clothes, sometimes without their parents present and rarely with consent. Sometimes as adults they would find these pictures of themselves in medical journals, with black bars across their eyes. The black bars to supposedly hide their identity, but also as a way of saying that who they are doesn’t really matter, they are just a body to be marvelled at as a medical wonder. A slide to be shown in a medical lecture, with all the ‘oohs and ahhs’ as the students realise the female looking children have XY chromosomes.
Until recently, I only ever saw these pictures in medical journals or older medical textbooks and I was relieved to see that they were not present in my copy of ‘The Illustrated Textbook of Paediatrics’ that I read from cover to cover whilst at medical school. Until recently, I had hoped these pictures had become a thing of the past and that we were now less likely to treat people in this dehumanising way, reducing them to just a curiosity in a textbook. However, I am now increasingly seeing these pictures used on Twitter as a way to validate beliefs in gender identities and that a woman is anyone who identifies as a woman. These pictures of intersex women like me are supposed to prove that being a woman is a feeling – and that if I can be accepted as a woman, anyone should be accepted as a woman. The dehumanised bodies of people like me have become the ultimate ‘gotcha’ in debates about gender identities.
However much I feel I have made peace and accepted the things that have happened to me – and however much I now feel that I have a happy and fulfilling life, filled with friends and family, there is something gut wrenching about seeing these pictures used in this way. A visual sign of the trauma, isolation and stigma that so many of us born with different bodies have experienced. As many celebrities and academics cheer along and claim to be on ‘the right side of history’ in the gender wars, little thought is given to the treatment of intersex people who have been caught in the middle. This needs to change if we are ever to really help children with different sex development get the help they need, to grow up without secrecy and shame.
Although I am always meaning to write something about my experience as a woman with Androgen Insensitivity Syndrome, I am also a terrible procrastinator and with work and kids to juggle, a few tweets are usually the limit of my attention span. Before starting this piece, I was also worrying about the best terminology to use to define myself, as even this has become a minefield. Should I call myself intersex, or am I better defined as someone with a difference in sex development (DSD) or variation in sex characteristics (VSC)? However, over the last few weeks I’ve felt that it has become increasingly important to write something, even if I use these terms interchangeably.
Intersex lives have again been thrown into the many debates raging on Twitter about what it means to be a woman and my thoughts and position seem to be constantly misrepresented or vilified. I have even seen my biology used to accuse JK Rowling of supporting the mutilation of intersex baby’s genitals and to compare her to Jimmy Saville and to validate the most horrific abuse as recorded here https://medium.com/@rebeccarc/j-k-rowling-and-the-trans-activists-a-story-in-screenshots-78e01dca68d. Her crime has been to write the below tweet and an essay on her experiences as a woman. https://www.jkrowling.com/answers/
The toxicity of this debate has resulted in even well-respected academics who write about intersex issues, endorsing the belief that it is acceptable to refer to people like me in the most dehumanising ways. This has even included calling the only charity in the UK working with children with different sex development, ‘trash’. This has been deeply upsetting for those of us who work with children and families who are facing these incredibly complex issues.
As a woman born with Complete Androgen Insensitivity Syndrome, Twitter is a difficult place. There are now frequent arguments about what it means to have an intersex body. On one side there are the debates about intersex women competing in sports and frequent comments such as “women’s sport is only for XX women” and even wanting to remove me from the sex classification I was given at birth. On the other side, I am referred to as a hermaphrodite or described as a third sex or neither male or female – and my body is used to validate the most horrific abuse of women or to prevent women from talking about their own biological experiences. I have witnessed my intersex body being used to validate rape and death threats being directed at women who want to discuss their sex based rights. This has even included using my history to validate the homophobic abuse of lesbians who define themselves as exclusively attracted to women. When I have asked for my biology not to be used in this way, I have been called ‘trash’, a freak and even a TERF, a term that has now become the easiest way to dehumanise a woman for her opinions.
I have repeatedly been called transphobic for asking that intersex people are not conflated with trans identities, as this silences our voices, causes public confusion about our needs and concerns and even leads to the groups that support us losing out on desperately needed funding. I have been told that I am a right-wing authoritarian in league with white supremacists, mainly because I think it is important to listen to the voices of mostly left-wing women in the UK, with long histories of social justice activism and working with vulnerable people. These are absurd accusations and are similarly used to silence many women and their groups.
I believe that anyone who identifies as trans should be supported and free to live without stigma and discrimination – and I fully support any adult who chooses to transition, if this allows them to live in the way that is best for them. However, I also believe that I deserve my voice to be heard and my own story to be told.
The persistent online othering of intersex people
There is now a narrative that is continually repeated on social media, that states intersex people are neither male or female or a third, fourth or even fifth sex. This is frequently repeated by people with no experience of intersex issues and these messages often include inaccurate information about our lives and bodies and frequently include discussions of our genitals, even referring to us as having “both sets of genitals”. When trying to correct these misrepresentations, I am frequently dismissed, blocked or called transphobic. It frequently feels that I have become nothing more than an interesting anecdote someone has learned about in a gender studies lecture – and they have not considered that people like me really exist & should be offered the same respect as everyone else. We should not have our lives weaponised and used as part of a thesis, especially by people who have no interest in listening to our voices and will immediately block us on social media, if we do not agree with their analysis of our bodies.
I agree that we have complex biological variations that do not sit neatly into binary boxes – and this can be incredibly distressing and isolating for newly diagnosed children and families. People talk about intersex people being as common as red hair, but in reality, it is only a tiny number of children and families who are facing these really complex issues. In the UK, only around 150 children are diagnosed with a difference in their sex development each year, which means there is unlikely to be another parent in your NCT group experiencing the same issues – and there is unlikely to be another child in your school or sometimes even in your town. Parents frequently feel terrified and alone – and the othering language that is persistently used to describe their children, is likely to only increase their feelings of isolation. If children with different sex development are to grow up without stigma, secrecy and shame, we need to ensure that their parents are well supported and treated with compassion and sensitivity. By supporting parents, we are giving them the best chance to be positive advocates for their children.
There are now numerous guides for schools that talk about the best practice for supporting transgender young people. These all talk about the trauma of being misgendered or the pain that can be caused by not respecting pronouns. We are told that not affirming someone’s gender is an act of violence and can lead to young people attempting suicide. The latest advice from Stonewall also talks about “listening to the child or young person and following their lead and preferences”. The Trans Inclusion Toolkit from Allsorts states “Follow the lead of the child, young person and if appropriate their family”.
It is hard to understand why people promoting these guides on how to best support trans young people, do not share the same empathy for children & young people with different sex development. One recent comment stated that those of us arguing that it is wrong to force a third sex narrative onto all intersex people, have a “fear of being othered away from our female safety nets”. This seemed to dismiss any of the trauma & real loss that many intersex women have experienced. Born and raised as girls and then finding out as young teens that they could not have children & could have difficulty having sex due to lack of vaginal depth – as well as finding out about your chromosomes and internal testes. You do feel ripped away from everything you thought was true about yourself. It takes time to process this and grieve for these very real losses, before being able to put yourself back together again in a way that you can feel positive about living with a different body. This can take time and patience and it is essential that anyone working with children and families facing these issues, is able to be compassionate and sensitive to their needs. The current trend to other intersex people as a third sex or neither male or female, offers newly diagnosed children & families, none of the same empathy and understanding that is considered vitally important when supporting young people with gender dysphoria. Information sent to schools, often includes the Genderbread Person or Gender Unicorn, which has intersex listed as a third sex, alongside ‘other’. The Allsorts Toolkit references intersex, although the information they provide is misleading and even inaccurately implies that many intersex people transition as they have been misdiagnosed in infancy.
I want people with differences in their sex development to have the freedom to define themselves in the way that is best for them – & to talk about their own experiences in the way that feels most authentic. For some, this may be defining themselves as having a medical condition and believing that they shouldn’t feel stigmatised by this, any more than they should feel stigmatised for having diabetes or asthma. They may want to work with health professionals to try and improve care for children and young people. For others, especially people who have experienced traumatic & non-consensual surgery, any dealing with health professionals is difficult. I can also understand that an intersex identity can be an important way for some people to reclaim ownership of their lives and body – and I fully support any intersex person to talk about themselves in this way. It is also amazing to see young intersex activists proudly talking about their bodies and experiences and trying to form connections and support networks with other young people. This is so inspiring for young people growing up with different bodies and can show them that they don’t have to feel ashamed or alone. Our bodies do not need to be fixed and are usually healthy and fine to be left alone.
What I don’t support is trying to force the third sex narrative onto all of us born with different bodies – and I am now seeing even women with PCOS and men with mild hypospadias having their biological sex questioned & debated. It is important to recognise that we may need different narratives and perspectives at different times of our lives and that we are allowed the space to work this out for ourselves. Most important for me is that we speak out against the constant debates about the nature of ‘what we are’ and instead concentrate on ‘what we need’.
What do we need?
Intersex people are a diverse group and this is represented in our needs. However, most us have a sex easily identified at birth and learn to live with our different body & are happy to stay in the sex in which we grew up. Although a few intersex people may choose to identify in different ways, this is not a priority for most – and although sensitive and inclusive language is vital, pronouns and third sex markers are rarely a priority issue. There are rare occasions when it is extremely difficult to determine the sex of an infant or when a difference in sex characteristics can be associated with an underlying life threatening medical condition. These children and their families should not have their complex histories used or weaponised, without any consideration to the significant trauma they will possibly have experienced.
From my own perspective, our main priorities are as follows:
Good psychological support for children & their families. This is vital if parents are to be supported to be the best advocates for their children. They need support to ask questions about any intervention that is recommended & to know that surgery isn’t necessary unless there is an urgent clinical need. It is vital that they know it is OK to wait and to be offered the psychological support to help them discuss what is happening with friends and family.
Any medical or surgical intervention offered should have robust evidence and consider the long-term risks and complications. As with all types of surgery, this should be considered only when there is clinical need. Do no harm should be prioritised for any intervention.
Age appropriate information, stories & narratives should be available to support young people to describe their experiences in the way that is best for them. These may need to be culturally sensitive and presented without judgement.
Peer support for young people, so that they understand it is OK to grow up with a different body and that it is OK to ask questions. They also need to be given honest and accurate information about their body.
Allowing children & families to talk about their experiences in their own words and feeling that there are supportive places where their voices can be heard.
Good medical care to support the very real medical complications that people with differences in their sex development can commonly experience. This can include hormone levels, HRT, bone density, lack of vaginal depth, infertility and even hearing problems.
Support for young people as they go through puberty & start to explore the possibility of sex and relationships. This may include the use of dilators to increase vaginal depth & can require significant emotional support.
We need more tolerance of different views amongst intersex people, so that we can feel comfortable to discuss our lives, helping to reduce stigma by not alienating the people that are in the most need of support.
What we really don’t need is to be used, appropriated and even fetishised in debates about gender. This results in our own humanity being lost in endless discussions about ‘what we are’ or ‘how we are classified’, with very little concern about ‘how we are treated’. We should not be used as ‘gotchas’ in debates about gender identities and used to validate threats and abuse of women. We should not be forced to describe our experiences according to beliefs in gender identities, especially as not all of us experience this and feel we are as much a complex mix of masculine & feminine traits as any other human.
We should also not be used to validate the medicalisation of gender dysphoria in children. I believe that my body was surgically altered as a teenager, based on the ideological belief that my body must match my gender or gender identity, which correlates with the many stories I read today of children born in the wrong body and needing ever earlier intervention. My parents were even told that if I was given accurate information about my body, I would be suicidal – and therefore consented to all interventions suggested. I am not arrogant enough to claim that I have all the answers and it is likely that transition is in the best interests of some children and young people. From my understanding of what is currently happening in the UK, the Gender Identity Service (GIDS), still has many sensible voices that are calling for robust evidence and want to ensure careful assessment and psychological support. However, I am concerned about any groups that are trying to prevent open debate and are aiming to prioritise their ideological beliefs over the evidence. This has the potential for significant harm, very similar to the harm experienced by many intersex people.
Do these views, which I would not consider extreme, hateful, violent or intolerant – mean that I should be dismissed as transphobic & dehumanised as ‘trash’ or a TERF? Have people become so intolerant, that even asking to have our own voice can lead to this abuse? Has this debate become so toxic, that even discussing the very real ethical considerations involved with medical interventions in children, including sterilisation, can result in you being treated in this way? It has been especially distressing to see people who claim to speak and work with intersex people, endorsing this language – and treating some of us as if we are ‘the wrong sort of intersex people’.
Most importantly, we need to remember that there are children and families experiencing these very real and complex issues – and it is vital that their wellbeing and needs are not lost in this never ending and increasingly toxic debate.